|

|
There are less frequent forms of atypical spondyloarthritis generally characterized by predominant osseous inflammation and often associated with dermal diseases, most frequent pustulosis palmoplantaris. Such changes have often been termed Pustulotic arthro-osteitis (PAO) or SAPHO (Synovitis, Acne, Pustulosis, Hyperostosis) and when occurring in children CRMO (chronic recurrent multifocal osteomyelitis). Recently the term CNO (Chronic non-bacterial osteitis) have been introduced to cover this spectrum of relatively rare auto-inflammatory conditions sharing musculoskeletal and cutaneous manifestations. The disorders are characterized by non-infectious chronic osteitis, involving both the cortical area and the bone marrow with characteristic endosteal as well as periosteal new bone formation resulting in sclerosis and hyperostosis. Polyostotic involvement is frequent, especially in children/adolescents, doi:10.1055/s-0038-1639469. |
| |
The site of disease involvement is age-related. In adults, the sterno-costo-clavicular region is the most common location followed by the spine and SIJ whereas the metaphysis of long tubular bones, the spine and clavicles are most frequently involved in children/adolescents, doi:10.3899/jrheum.181254; doi:10.1016/J.SEMARTHRIT.2018.09.004. |
| |
|
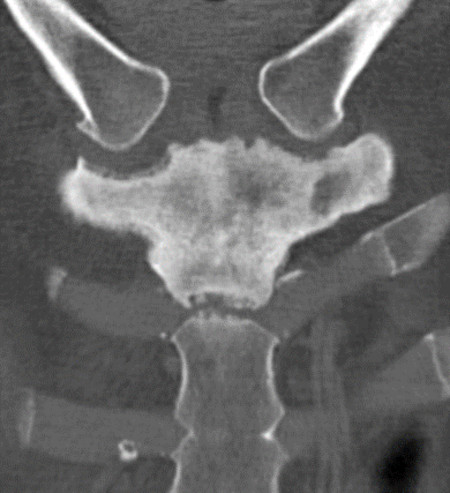
CNO changes at the SIJ are most frequent in adults where they are often unilateral and confined to one of the bones, most common the iliac bone, doi:10.1016/J.CRAD.2011.08.014.
The MRI appearance depends on the stage of disease. During active stages, there is BME and enhancement whereas chronic changes are predominantly characterized by sclerosis and hyperostosis with concomitant fat metaplasia in the bone marrow corresponding to previous BME areas. The diagnosis is often be based on a combination of clinical and radiologic findings, but supplementary biopsy may be needed in case of tumor-suspected lesions.
|
Semi-coronal CT slice in an adult with pustulosis palmoplantaris showing increased bone density corresponding to the left-sided iliac bone adjacent to the SIJ (arrow). |
|
Semi-coronal post-contrast T1FS image shows pronounced enhancement in the diseased area as a sign of activity. Moreover, enhancement in the sacrum beneath the vertebral plate at L5/S1 without accompanying changes corresponding to the 5th lumbar vertebra or the disc (arrows). |
|
| |
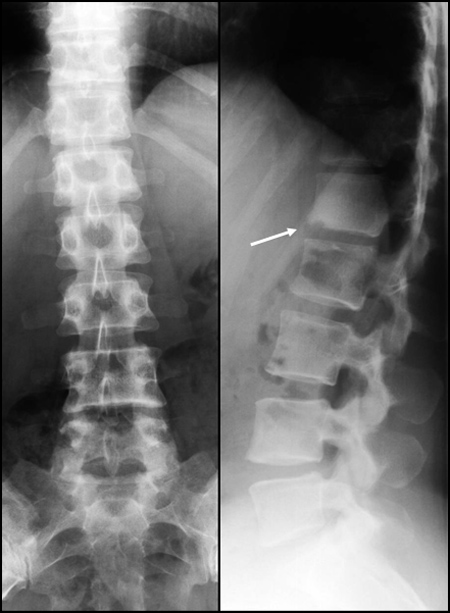
The changes often involve several vertebral bodies, which during active phases display edema by MRI. Typically, gradually increased bone density develops and there may be erosion of the adjacent vertebral plates, often without accompanying disc involvement. |
|
Sagittal T1 and STIR image show osseous edema in several vertebral bodies (arrows). There is also a small erosion at the lower vertebral plate of the first lumbar vertebral body. |
|
|
Simultaneous radiography, frontal and lateral view, only shows changes in the lower part of the first lumbar vertebral body in the form of increased bone density and the erosion also visualized by MRI (arrow). |
|
| |
|
Involvement of anterior chest wall (ACW) bones is a frequent finding in adults with CNO. Initially, the changes are usually confined to bones, displaying signs of activity which during the course elicit the development of osseous sclerosis and hyperostosis. The adjacent joints facets may be irregular initially and during the course the inflammatory changes may cross ACW joints resulting in involvement of bones on both sides of the joints. |
|
CT of the sternocostoclavicular region in a patient with pustulosis palmoplantaris and recurrent ACW pain. There is characteristic osseous sclerosis and hyperostosis corresponding to the manubrium sterni extending across the first sternocostal joints to the costal cartilages. |
|
| |
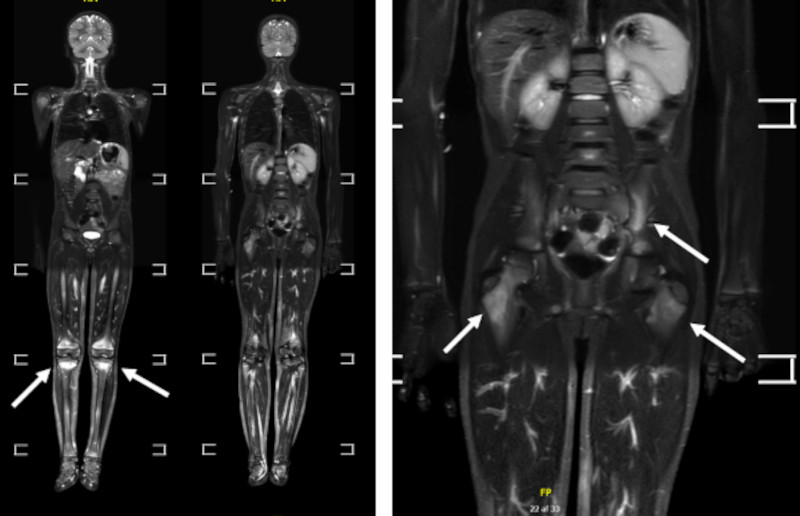
In childhood, CNO lesions at the SIJ will often be part of a multifocal osseous disease with accompanying lesions in other pelvic bones or in other skeletal areas. Whole body MRI is therefore a preferred examination in children/adolescents to detect symptomatic as well as clinically silent lesions, doi:10.1186/s12969-022-00746-y.
CNO lesions in the spine usually presents as BME in vertebral bodies which may be fragile implying a risk of collapse as shown beneath. |
| |
|
Whole body MRI, coronal STIR images with enlargement of the pelvic region to the right in a 10-year-old boy with CNO involving the left iliac bone with concomitant lesions at both knee regions and the proximal femoral bone adjacent to the greater trochanter (arrows). |
|
|
|
Spinal lesions in a 12-year-old girl, sagittal STIR images, to the left initially and to the right one year later during a quiet period. There is initially BME corresponding to the second lumbar vertebral and the second and third thoracic vertebra (arrows). One year later the signs of activity have disappeared, but the third thoracic vertebra has become wedged shaped due to anterior collapse (open arrow). |
|
| |
|
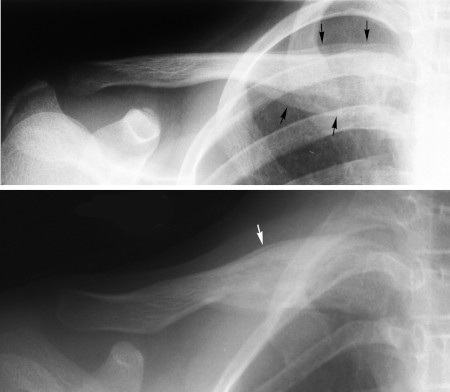
There may also be concomitant anterior chest wall changes in childhood, usually confined to the clavicular bone in the form of osseous inflammation with periosteal new bone formation which may be huge making the changes simulate tumor. However, by MRI there is often a bone within bone appearance due to the huge periosteal new bone formation.
During the course the periosteal new bone formation will ossify and be incorporated in the clavicular bone which will be sclerotic and increase in size. However, during a usually fluctuating course there can be exacerbation with the formation of periosteal new bone on the hyperostotic sclerosed bone as illustrated below.
|
|
Radiographs in a 8-year-old child with pain and swelling at the right clavicle. Upper image shows the initial examination with active periosteal new bone formation (black arrows) and the lower image one year later where the clavicle is hyperostotic and sclerosed, but with a slim periosteal new bone formation superiorly (white arrow) as a sign of activity. |
|
|
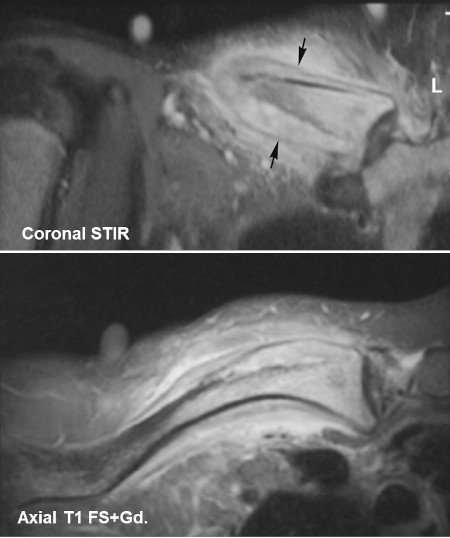
MRI, initially, coronal STIR and axial postcontrast T1FS, showing a typical bone within bone appearance due to a huge periosteal new bone formation (arrows) with concomitant pronounced edema and enhancement in the surrounding soft tissue. |
|
| |
|
|
|
|