Irrespective the stage of the disease, there are typical locations for active inflammatory and structural spinal changes in AS by MRI encompassing:
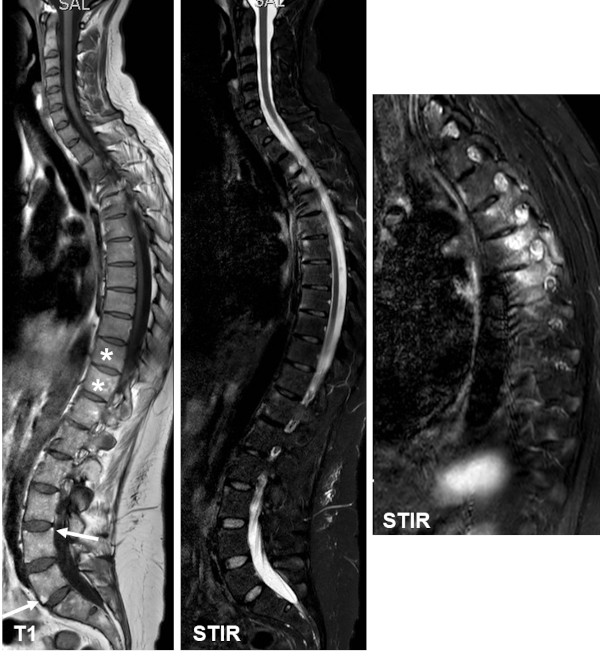
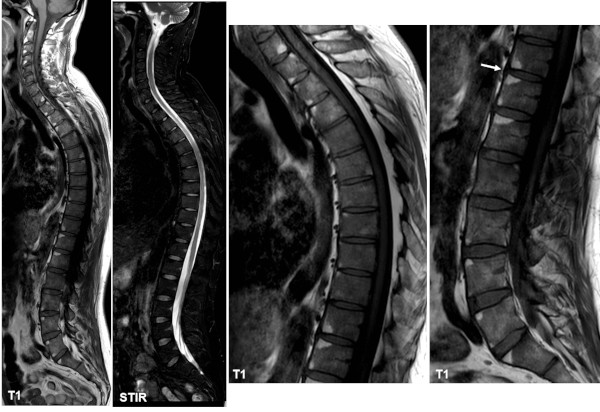
· BME/osteitis and/or fat deposition at vertebral corners, located to one or more of the four vertebral corners on sagittal images
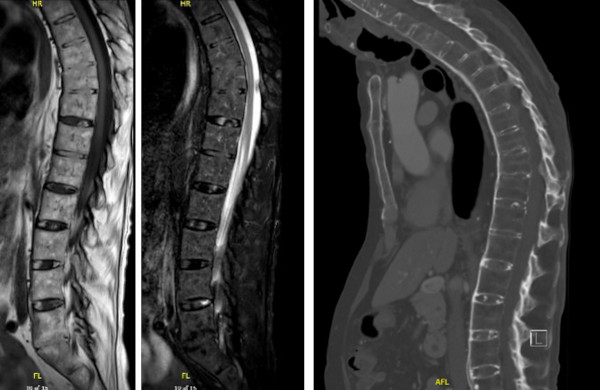
· Syndesmophytes new bone formation between vertebral corners; may only be visible by MRI if edematous or containing fat
· Spondylodiscitis (involvement of intervertebral discs) with BME and/or fat deposition located in the bone marrow adjacent to the intervertebral disc
· Arthritis of apophyseal joints, usually associated with bone marrow edema in vertebral pedicles
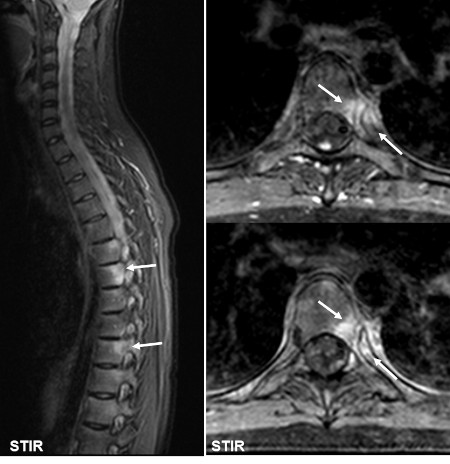
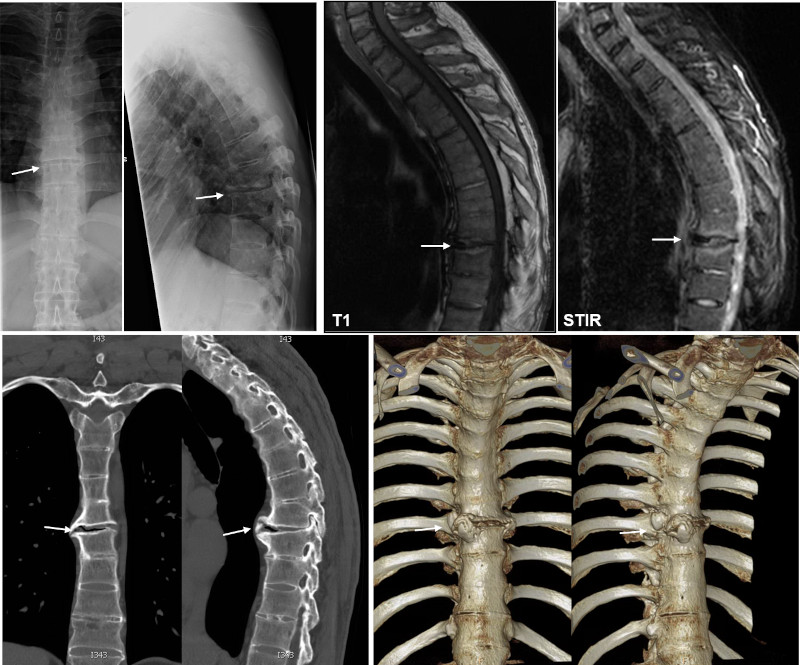
· Arthritis of costovertebral joints between the posterior lateral aspect of vertebral bodies and the ribs, usually with changes extending to pedicles and posterior aspect of vertebral bodies
· Arthritis of costotransverse joints lateral to the vertebral bodies with involvement of the rib and transverse vertebral process
· Enthesitis of spinal ligaments such as the supraspinal and interspinal ligaments
· Ankylosis/vertebral fusion - new bone formation within the intervertebral disks occurring in long-standing disease. |