|
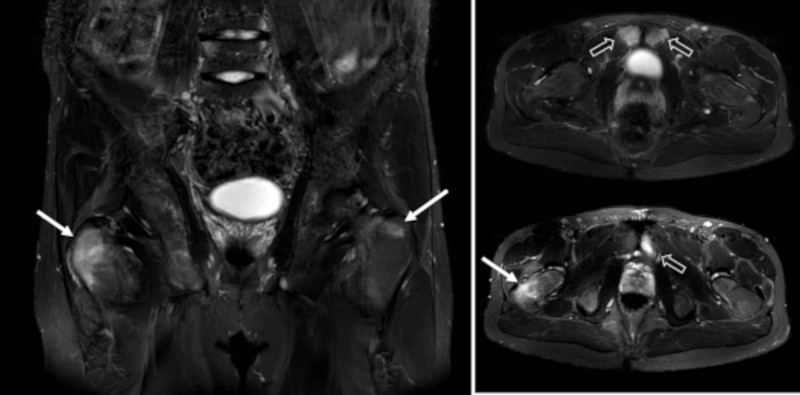
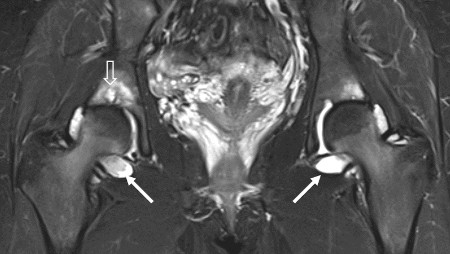
MRI, coronal and axial STIR images in a patient with bilateral sacroiliitis showing active enthesopathy changes at the greater trochanter on both sides (arrows), most pronounced on the right side. There is also osseous edema at the pubic symphysis (open arrows). |