The sequences used routinely in axSpA consist of:
T1-weighted semi-coronal sequence which is sensitive for detecting marrow fat signal appearing bright whereas fluid is black. Abnormal fat deposition, which can occur as a sequel after bone marrow inflammation, is well visualised on a T1-weighted sequence. Besides, a T1-sequence is optimal with regard to visualization of the anatomical structures. Fatty tissue is present between soft tissue structures such as muscles, which will therefore be clearly delineated.
Semi-coronal cartilage sequence such as a T1-weighted fat-suppressed (T1FS) sequence or a gradient echo sequence visualizing the bone cartilage interface (articular surface) to optimize the visualization of erosions.
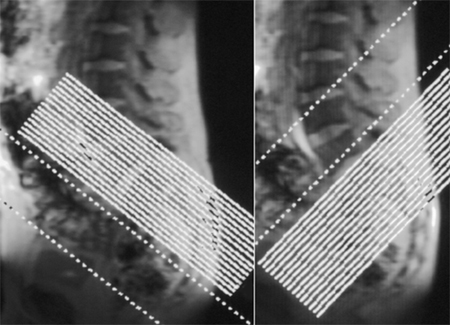
STIR (Short Tau Inversion Recovery) sequences or T2-weighted fat-suppressed sequences in two perpendicular planes (semi-coronal and semi-axial, respectively) to detect active inflammation, displaying areas with high water content bright against a slightly variable dark background due to suppression of signals from fatty tissue, doi:10.1136/ANNRHEUMDIS-2022-EULAR.3365.
In the case of suspected infection additional postcontrast T1FS sequences in two perpendicular planes are necessary to detect possible abscess formation etc., but in the evaluation of axSpA changes postcontrast sequences do not add diagnostic value to the sequences mentioned above, doi:10.3899/jrheum.090519.
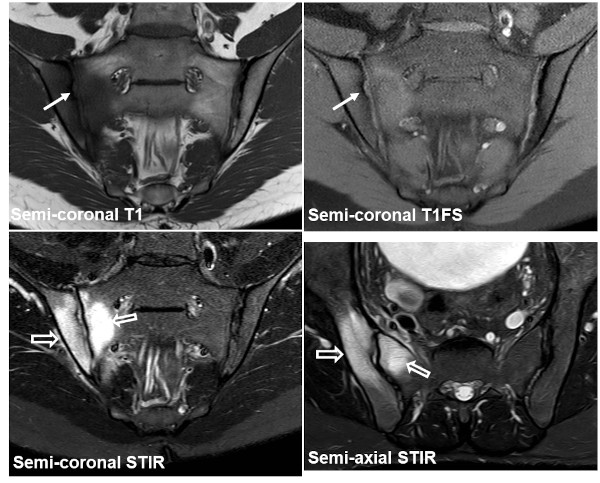
The images below show the recommended sequences, semi-coronal T1, T1FS and STIR in addition to a semi-axial STIR sequence. There is manifest subchondral edema at the right SIJ (open arrows) and also an iliac erosion (arrow), but no abnormal fat deposition. |